A brain stroke can arrive without warning — a sudden interruption of blood flow that throws the brain’s finely tuned circuitry into confusion. A stroke is sudden and frightening and leaves families scrambling to understand the brain stroke symptoms and brain stroke causes that led to it. One of the most commonly asked questions I hear from patients and carers is: “Does it matter whether the stroke was on the left or the right side of the brain?” The short answer is yes — the side (or hemisphere) affected shapes the kind of problems a person experiences, the rehabilitation focus, and how quickly others notice the event. In this blog, I’ll explain the typical differences between stroke left side paralysis and right sided stroke symptoms that often hamper the everyday life of the patient suffering and their caregivers associated with them.
How the Brain’s Halves Differ
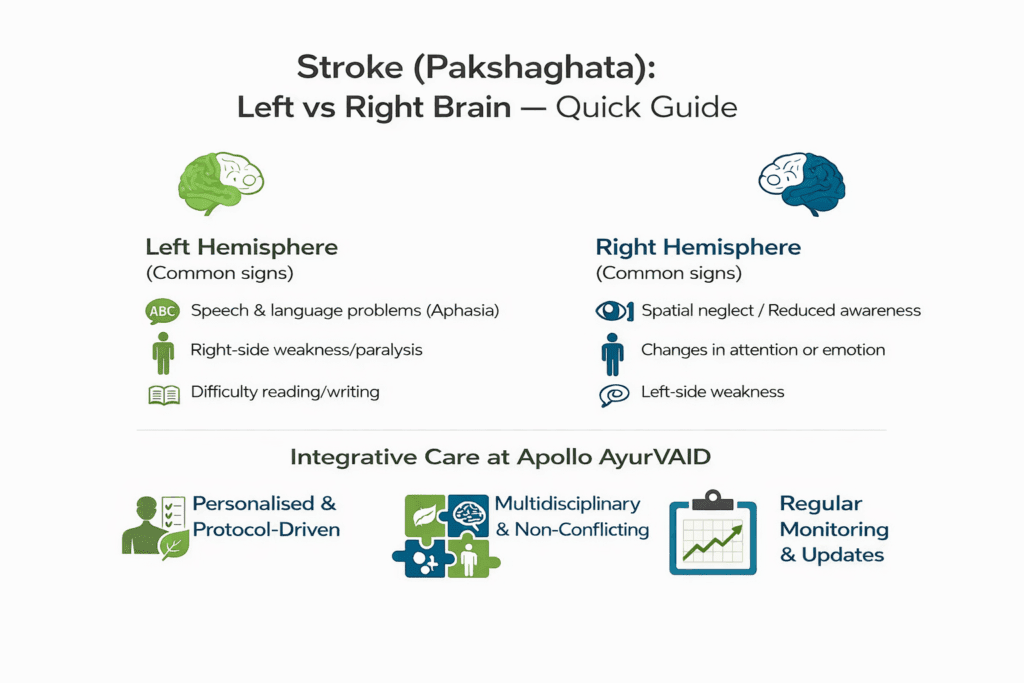
The two cerebral hemispheres share many jobs, but each has its own specialities. For most people, the left hemisphere plays the leading role in language, speech production, understanding, reading, and writing— so when a left-sided stroke occurs, language problems (aphasia), difficulty finding words, and trouble understanding speech are common. Such impairment often makes the stroke immediately obvious to family, emergency staff, or bystanders because the person may be unable to speak or follow commands.
By contrast, the right hemisphere is often more engaged in visuospatial awareness, attention, emotion perception, and monitoring the self and environment. Right-sided strokes can therefore cause problems like hemispatial neglect (not attending to the left side of space), impaired perception of body position, or anosognosia (reduced awareness of one’s own deficits). Because these signs have more to do with perception and awareness than speech, right-sided strokes can be missed or diagnosed later, which may delay the treatment.
Typical Clinical Features
Left-hemisphere stroke commonly presents with:
- Sudden weakness or paralysis of the right side of the body (contralateral motor deficits), often described as stroke left side paralysis – the words people use when looking up this issue.
- Speech problems: slurred speech, difficulty finding words, and poor comprehension (aphasia).
- Reading and writing difficulties.
Right-hemisphere stroke commonly presents with:
- Weakness of the left side of the body (left hemiparesis)
- Right sided stroke symptoms often point to confusion, reduced awareness of deficits, or ignoring the left side (neglect).
- The symptoms often include visual-spatial disorientation, difficulty judging distances, emotional blunting, and changes in behaviour.
Practical Differences for Families and Caregivers
- If a loved one has trouble speaking or finding words after a stroke, think left-hemisphere involvement and get urgent care.
- If a person seems oddly unconcerned, bumps into objects on one side, or dresses only one half of their body, suspect right-hemisphere stroke and assess for neglect.
- Safety planning matters early: patients with neglect may try to move unsafely and require supervision, while those with aphasia need alternative communication methods and careful explanation of care plans.
Why Right- and Left-sided Strokes are Sometimes Missed or Misjudged
Because the standard acute stroke scale emphasises language and command, left-hemisphere deficits are often easier to detect quickly. Right-hemisphere problems — especially neglect and unawareness — require specific tests and careful observation. If a person denies a deficit or appears “fine” verbally, family and clinicians must still watch for subtle signs, such as bumping into objects on one side, failing to eat from half the plate, or difficulty orienting while walking. Early recognition matters because treatments (like thrombolysis or thrombectomy) and rehabilitation planning are time-sensitive.
Left- or right-sided strokes—both situations call for clear, calm communication, reassurance, and teamwork with therapists. Remember: recovery can be slow and non-linear; grief, anger, and relief are all normal emotions for families and patients alike.
The Ayurveda Approach

How Integrative Care at Apollo AyurVAID Supports Recovery
At Apollo AyurVAID, stroke rehabilitation is intentionally integrative—it blends evidence-based Ayurveda principles with modern neurological rehabilitation so that patients receive the best of both worlds: root-cause-focused therapies plus standardised functional rehabilitation. The program is personalised, protocol-driven, and coordinated with the patient’s neurology and medical team. Key features include:
- Timing & patient selection — Rehabilitation begins once the patient is medically stable, usually after the acute phase (commonly 7–10 days post-event), and is most intensive during the early “golden” months of recovery. The team carefully assesses who will benefit most (medically stable patients in early or moderate recovery, those with residual motor/sensory deficits).
- Classical Ayurveda therapies tailored to strokes — Treatments frequently used within the protocol include therapeutic Vasti (enemas), Nasya (nasal administration of medicines), Shirodhara, Virechana (where indicated), and localised medicated oil therapies. These aim to pacify deranged Vata, nourish Majja dhatu (nervous tissue), reduce spasticity, and support neural repair.
- Modern rehabilitation is integrated seamlessly — Physiotherapy, occupational therapy, and speech–language therapy are core components; these are combined with Ayurveda modalities so that motor relearning, gait training, balance work, and communication therapies proceed alongside systemic Ayurveda care. This multidisciplinary approach addresses function (how patients perform daily tasks) and the underlying systemic barriers that can slow recovery.
Rehabilitation — Tailored to the Deficit
Timely stroke unit care, Ayurveda interventions, speech therapy for aphasia, and tailored occupational/physical therapy for motor and perceptual deficits are cornerstones of recovery.
Rehabilitation is individualised. Language therapy (speech-language pathology) is central for left-hemisphere strokes; for right-hemisphere strokes, occupational therapy that targets spatial scanning, prism adaptation, and attention retraining can be transformative. Early mobilisation and family involvement improve compliance and outcomes.
Final Notes
If you suspect a stroke—either speech stops on the left, or awareness fades on the right— act immediately. The sooner medical teams evaluate the person, the better the chance for treatments that reduce long-term disability. After the acute phase, a tailored rehabilitation plan that addresses the hemisphere-specific deficits will give the best chance of meaningful recovery. As a clinician and fellow human, I know how raw this time feels; you do not have to navigate it alone. Seek a stroke team that listens, explains clearly, and partners with you in every step of recovery.